florida blue appeal form
Accredo Prescription Enrollment Form. The Florida Blue temporary plans 6 mths are a scam.

A Deeper Look At Florida S Dangerous Transgender Medical Care Ban Legislation Equality Florida
Member Grievance and Appeal Form Mail to.
. Ancillary Request to Participate Form. Please describe the issue in as much detail as possible. Member Appeal and Grievance Form Mail to.
If you are deaf hard of hearing or have a speech disability dial 711 for TTY relay services. Medicare Appeals and Grievances Department PO. REQUEST FOR MEDICARE PRESCRIPTION DRUG COVERAGE DETERMINATION This form may be sent to us by mail or fax.
Determinations 1305 Corporate Center Dr Eagan MN 55121. The local office at River City Marketplace in Jacksonville Fl offered nothing but lip service. Check the applicable box on the Provider ReconsiderationAdministrative Appeal form.
Supporting documentation must be submitted. To submit a prior authorization online please click the button below to use the web form. Health Plan Grievance Appeal Form Non-HMO Used to appeal a coverage decision and request formal written review of how a claim was processed.
835 Health Care Electronic Remittance Advice Request Form. Florida BlueFlorida Blue HMO PO Box 41609 Jacksonville FL 32203-1609 Attn. You can pay 350 per month and they cover virtually nothing.
The following documentation is. FORMULARY EXCEPTION PHYSICIAN FAX FORM. Florida Blue and Florida Blue HMO Prescription Drug Benefits are administered by Prime Therapeutics our pharmacy benefit manager PBM.
This form is notintended for use in filing an appeal with a. 1-800-955-8770 to request this information. BlueDental Care - Form ID.
Appeals must be submitted within one year from the date on the remittance advice. You can contact us at 1-800-926-6565 TTY users. Box 1798 Jacksonville FL 32231-0014 Administrative Appeals.
You can find detailed instructions on how to file an appeal in the Disputed Claims Process document. Billing Authorization for Professional Associations. Florida Blue members take full advantage of your insurance plan.
Use this form to initiate a grievance or appeal PLEASE PRINT OR TYPE Please complete all information requested below. I hereby request a review of the Grievance or Appeal described below and understand that the receipt of this Grievance and Appeal Form by Florida Blue constitutes a request for review by the Local Office. BlueDental Choice - Form ID.
Supporting documentation must be submitted. The prefered method for filing the appeal to your. Florida BlueFlorida Blue HMO PO Box 41609 Jacksonville FL 32203 -1609 Attn.
Use this form to select an individual or entity to act on your behalf during the disputed claims process. You may also ask us for a coverage determination by phone at 1-800-926-6565 800 am. Check the Adverse Determination box under Appeal Type.
Care Management Referral Form. Member Appeals Appointment of Representative AOR Form. Access Authorization Unit PO.
Find all your forms for prescriptions claims and more all right here. GroupPlan on ID Card. For other language assistance or translation services please call the customer service number for your local Blue Cross and Blue Shield company.
I acknowledge that Florida Blue Florida Blue HMO andor Truli for Health coveragemembership is contingent upon the. Authorized Representative Designation Form. Select Providers then Provider Manual.
Florida Blue Prior Authorization Form PDF 2019-2022. Member Grievances Appeals Fax. You may mail or fax it to the addressfax number provided above.
Self-insured Plans - Form ID. Mail the form and supporting documentation to. Click on the applicable form complete online print and then mail or fax it to us.
Use a florida blue prior authorization 2019 template to make your document workflow more streamlined. Please describe the issue in as much detail as possible. Y0011_33247 0216 GA CMS Accepted.
Medicare Advantage Member Grievances Appeals Fax. When an overpayment is made I authorize Florida Blue Florida Blue HMO andor Truli for Health to recover the excess from any person or entity that received it. Accordingly I authorize persons or entities that have any medical or other records or knowledge.
Florida Blue - Health insurance. Florida Blue Health Plan Appeals Jacksonville FL 32231-4197 Health Plan Grievance and Appeal Form I understand that in order for Florida Blue to review my appeal they may need medical or other records or information relevant to my appeal. I understand that in order for Florida.
Upon request Medicare Advantage plans are required to disclose grievance and appeals data to Medicare Advantage enrollees in accordance with the regulatory requirements. Mail the form and supporting documentation to. Please read and sign the statement below.
Box 41629 Jacksonville FL 32203 -16 29 Fax. Florida Blue is an Independent Licensee of the Blue Cross and Blue Shield Association Y0011_20892 1213R3 GA CMS Approved Y0011_20892 1213R3 GA EGWP C. Please read and sign the statement below.
Blue Cross and Blue Shield of Florida. Prime Therapeutics LLC 1-800-693-6703. ONLY the prescriber may complete this form.
Please read and sign the statement below. If necessary use additional sheets. Disputed the bills I recieved month later and never got a response.
I hereby request a review of the Grievance or Appeal described below and understand that the receipt of this Grievance and Appeal Form by Florida Blue Preferred HMO constitutes a. You may mail or fax it to the addressfax number provided above. Complete accurate disclosure of the information requested on.
This form may be used to appeal an adjudication examiners determination. Incomplete forms will be returned for additional information. Box 45296 Jacksonville FL 32232 PURPOSE SECTION I Please provide the following information regarding the person whose Protected Health Information is to be.
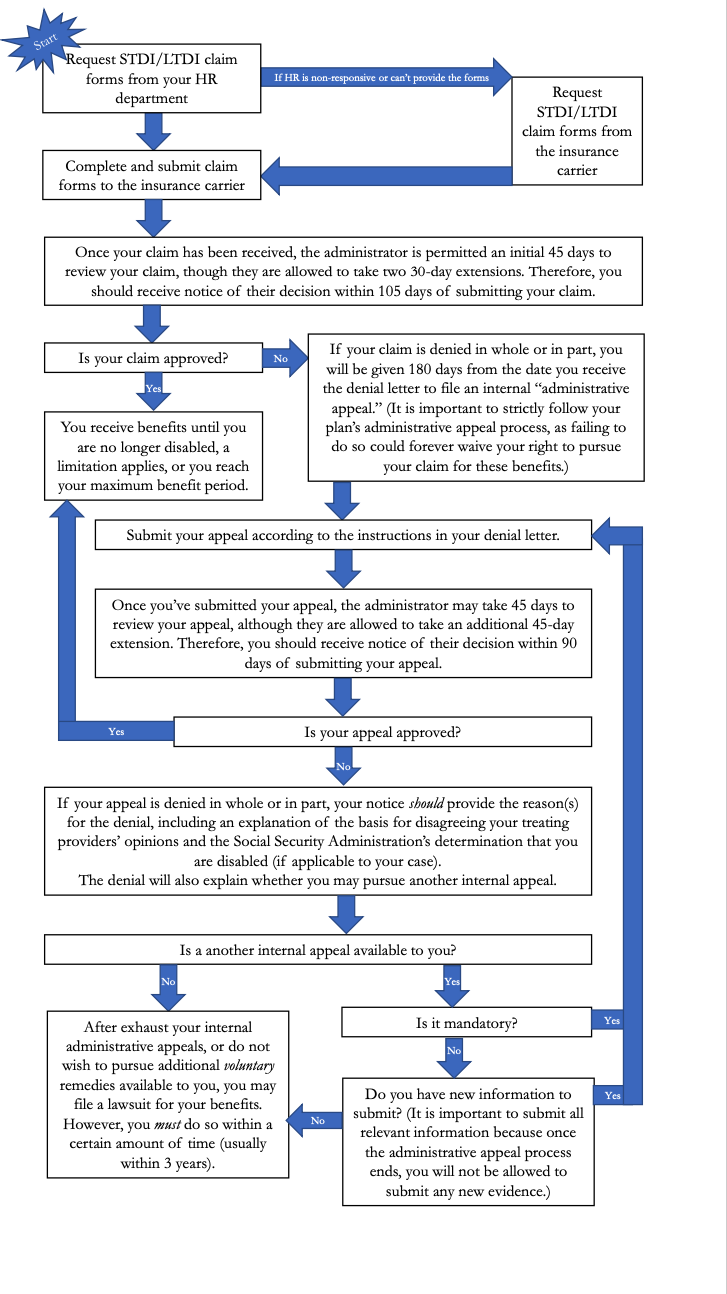
How To Claim Disability Benefits For Mental Health Conditions Hawks Quindel Website
2
2
George Packer The Four Americas The Atlantic

Florida Launches New Form To Report Unemployment Fraud
2

Florida Launches New Form To Report Unemployment Fraud

Tax Information Floridajobs Org
Consumer Appeal Rights In Private Health Coverage Kff

Free Prime Therapeutics Prior Rx Authorization Form Pdf Eforms

Florida Launches New Form To Report Unemployment Fraud
2

Fixture Seal Of Approval Application International Dark Sky Association
2
2
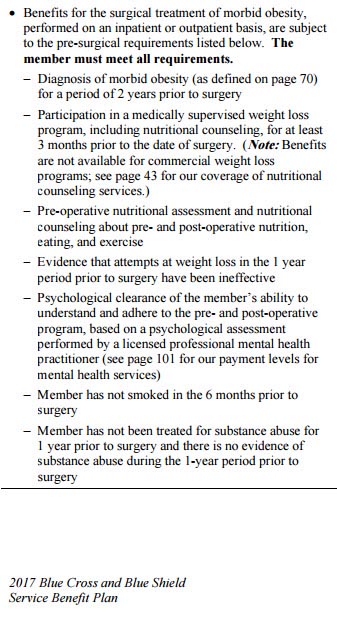
Bcbs Fed And Florida Blue S Weight Loss Surgery Criteria
2

4th Birthday Inflated Balloon Bunch Blue Balloons Personalized Balloons 4th Birthday
2